Now that you’re about a month into your child’s second year of life, you may have settled into a nice routine. At this point, your child has (hopefully) accepted whole milk (or a cow’s milk alternative) as a beverage, is eating cut-up table foods (while avoiding choking hazards), enjoys sleeping 11-14 hours per day (total), and loves to play.
While keeping your 1-year-old occupied can be exhausting, it can also be fun. Popular games at this age include playing peek-a-boo, pretending to talk on a toy phone, listening to music, reading lift-the-flap books (which kids inevitably rip), and stacking blocks.
One Game to AVOID Playing?
Pulling your child up by their arms and swinging them around, like so:
Why Does This Get the Thumbs Down? Because this game (though fun) can cause something called “Nursemaid’s Elbow.” Nursemaid’s Elbow is actually a pretty easy fix, but it hurts like the dickens.
Disease Spotlight: Nursemaid’s Elbow (Fancy Name: Radial Head Subluxation)
Nursemaid’s Elbow is a partial dislocation of the elbow. It occurs when the ligament holding the two bones of the forearm together slips out of place.
How Does This Happen?
This can happen when someone suddenly pulls up on a child’s arm. It’s commonly seen when parents:
Swing their child around by the arms.
Pick their child up by pulling up on their arms (vs. picking them up under the armpits).
Tug on their kid’s arm when helping them up on a curb.
Pull on their child’s arm while getting them dressed.
Insider Info: When kids get older, they can also get nursemaid’s elbow from playing on the monkey bars.
Who Typically Gets Nursemaid’s Elbow?
Children ages 1-4 years. 80% of cases occur in toddlers (kids 1-3 years).1
What are the Symptoms of Nursemaid’s Elbow?
Children with Nursemaid’s Elbow will cry and stop using the affected arm. In addition, they won’t want anyone to touch their arm or move it.
How is Nursemaid’s Elbow Diagnosed?
The diagnosis is typically a clinical one.
Doctors suspect Nursemaid’s Elbow when a child holds their arm in a certain way (bent at the elbow and close to the chest) AND when the parent reports a classic mechanism of injury (such as swinging the child around by their arms).
Insider Info:Some doctors will get an X-ray of the arm to make sure there’s no underlying fracture.
How is Nursemaid’s Elbow Treated?
Treating a Nursemaid’s Elbow is incredibly gratifying for pediatricians.
Why’s That?Because Nursemaid’s Elbow can be “fixed” by a simple maneuver that takes about 2 seconds.
Really! How?To do the maneuver, the doctor holds the child’s hand (like they’re going to shake it) and then either quickly twists the child’s forearm (“hyperpronates it”) or bends the arm towards the child’s chest. Different doctors have different techniques. Don’t try any of them at home, though — fixing a Nursemaid’s Elbow is more complicated than it looks.
Afterwards, your child will be able to move their arm like nothing happened and the doctor will look like a hero. It’s a win-win.
Insider Info:
Once the maneuver (aka the “reduction”) is performed and the Nursemaid’s Elbow is “fixed,” the child may still be reluctant to move their arm for fear that it will hurt. In addition, they may be mad at the doctor for yanking on their injured arm.
One of the tricks doctors use to see if the reduction worked is to offer the child a popsicle in an effort to get them to reach for it with the now “fixed” arm. If the child does, then they’re good to go.
If the maneuver doesn’t work the first time, the doctor may try it one more time or get an X-ray to make sure nothing else is going on.
Once a child gets Nursemaid’s Elbow, they’re at risk of getting it again. Therefore, if your child ever develops Nursemaid’s Elbow, be careful about tugging on that arm in the future and make sure to pick them up under their armpits.
The Bottom Line
Nursemaid’s Elbow is a fairly common occurrence in toddlers. Luckily, it can be treated quickly, leaving the doctor feeling quite pleased with themselves and the sheepish parent feeling relieved they didn’t accidentally break their child’s arm.
Celebrities Are Just Like Us!
“It just occurred to me that the majority of my diet is made up of the foods that my kid didn’t finish.”
~Carrie Underwood
The Reminders for This Week are the Same as Last Week’s. Get Wise About Them Below…
Limit Your Child’s Whole Milk to 16-24 Ounces Per Day.
Feed Your Child What You Eat, But Cut into Small Pieces.
Steer Clear of Choking Hazards. Get Wise About the Top 10 (Food) Choking Hazards Here.
Brush Your Child’s Teeth Twice a Day (Especially After the Last Meal of the Night) and Have Them Visit the Dentist Every 6 Months (Unless the Dentist Says Otherwise).
Call the Doctor If Your Child Spikes a Fever Above 102.2°FOR If They Develop Any Other Worrisome Symptoms (Such as Lethargy or Poor Feeding).
Continue to Give Your Child a Daily Vitamin D Supplement (600 International Units Per Day).
Keep Your Child in a Rear-Facing Car Seat Until (At Least) 2 Years of Age.
And…That’s a Wrap!
Welcome to Month 12 (Week 3) of Parenting Your Toddler!
Your child’s first steps mark a major milestone in both of your lives. Although doctors look for independent walking to occur around 1 year, some kids get the hang of it earlier, while others need more time.
In fact, only 50% of kids are independently walking by their 1st birthday, which means the other half are walking later than that. 90% of kids take their first steps by 15 months.1 Therefore, pediatricians don’t usually consider children to be “late walkers” until they’ve reached 15-18 months of age and haven’t taken any steps. At this point, the pediatrician will refer the child to a developmental-behavioral pediatrician and/or to a physical therapist for an evaluation.
Get Wise about the Top 10 Walking Tips & Truths in the Hot Topics section below. We’ll also discuss nosebleeds since new walkers tend to fall on their faces sometimes.
Diet:
Continue to offer your child cut-up table foods and introduce new foods (in a pressure-free way). Remember, it may take your child 10-15 tries to “accept” a new food, so don’t despair if some of your attempts end up on the floor.
Whether your child is crawling, cruising, or taking their first steps, it helps to know the following Tips & Truths About Walking. Get Wise About Them Below…
1. Know Your Terms.
Walking and “cruising” are two different things. A cruising child takes steps while holding onto furniture, whereas a walking child takes steps without holding onto anything. Cruising is a developmental milestone on the road to walking.
2. Slow and Steady Wins the Race.
Pediatricians like positive trends, so if your child crawled, pulled to a stand, and is now cruising, then walking is not far off.
3. Stay Cool.
Try not to pressure your child to walk.
Why? Because you don’t want it to turn into a power struggle. You can place a favorite toy just out of their reach for motivation, but don’t force it, and always offer assistance when needed or requested.
4. Birth Order May Matter.
First-born children tend to be more cautious when it comes to walking. Even though they’re perfectly capable of walking, they may want to hold a parent’s hand for extra support and will drop to their knees and crawl if the parent lets go. These are the types of kids who randomly walk across the room one day when their confidence is up.
One theory for why this happens is that first-born children model their walking on the way their parents walk and become a bit perfectionistic about it. Second-born children, on the other hand, see their older sibling as the role model, and aren’t as worried about making mistakes. Moreover, second-born children don’t want to be left behind. The exception to this rule is second-born children who are picked up so much they don’t have a chance to practice walking.
Another theory is that parents tend hover over their first child and are more laissez-faire with their second child.
5. Try Not to Fall Into the Comparison Trap.
Why?Because kids naturally vary in terms of when they reach their milestones. Moreover, parents often compare their children to other kids of slightly different ages. This is a faulty comparison, however, because even a month or two can make a big difference in terms of a child’s development.
6. Up Your Childproofing Game.
Although children tend to walk slowly and awkwardly at first, it doesn’t take long for them to pick up speed. There are certain safeguards that need to be in place before your child starts walking (many of which you’ve probably already implemented). These include (but aren’t limited to):
Ensuring there are baby gates at both the top and bottom of the stairs.
Plugging up electrical outlets.
Using corner guards to pad sharp furniture edges. In addition, you’ll want to secure all heavy furniture and TVs to the walls to prevent them from tipping over.
Installing window guards (which prevent windows from opening more than a crack). Make sure to tie up all window cord covers, too.
Locking up cabinets and drawers.
Scanning the floors and furniture for choking hazards.
PediaTip: If an item is small enough to fit inside a cardboard toilet paper roll, either hide it or get rid of it.
Removing breakable objects from surfaces (if you want to keep them in their unshattered form).
Putting covers on the doorknobs.
Making sure there’s a splash guard on the stove and covers on the knobs.
7. Say No to Walkers.
Avoid walkers (like the one in the picture below).
Why?Because they’re dangerous.
Note: Push toys like shopping carts and lawnmowers are okay, but keep them away from the stairs.
8. Don’t Fret About Your Child’s Future Athletic Career If They End Up Being a “Late Walker.” Late Walkers Can Still be Ballers!
“Late walking” doesn’t mean a child won’t be a good athlete. Early walking is actually more predictive of being a risk-taker than of becoming a pro athlete.
9. Skip the Shoes: Keep Your Child in Bare Feet at Home.
Why? Because kids like to grip the floor with their toes to “feel” each step.
10. Call the Doctor If Your Child Seems to Have a Strange Gait or Starts to Limp.
Most toddlers have a somewhat wide-based gait (forbalance) and look bow-legged. A small percentage will walk on their toes (aka “toe-walk”). This is often a normal phenomenon but, in some cases, can be associated with autism spectrum disorder, especially if other worrisome signs are present (such as poor eye contact, preferring to be in one’s own world, and seeming disinterested in people).
A common cause of limping in kids is toxic (transient) synovitis, which sounds scary but isn’t usually a big deal.
Toxic (transient) synovitis is a common cause of hip pain and limping in kids (especially in kids 3-8 years of age).
What is Toxic (Transient) Synovitis?
Inflammation of the hip joint.
What are the Symptoms of Toxic Synovitis?
Symptoms Include:
Fussiness: Kids with toxic (transient) synovitis are often super fussy and complain of hip pain (when they’re old enough to verbalize it).
Limping or Refusing to Walk Altogether.
What Causes Toxic (Transient) Synovitis?
Although the exact cause of toxic (transient) synovitis is unknown, it usually follows a mild viral infection (like a cold or a gastrointestinal bug).
Is Toxic (Transient) Synovitis Serious?
No. The name makes it sound worse than it is. Focus on the “transient” part rather than the “toxic” part.
How is Toxic (Transient) Synovitis Treated?
With anti-inflammatories (such as ibuprofen) and rest.
Nosebleeds & How to Manage Them
If your child takes a digger while practicing walking, they might get a nosebleed. Falling on one’s face isn’t the most common cause of nosebleeds, however. The No. 1 cause is actually NOSE PICKING. Dry air is a frequent contributor, as well.
Nosebleeds can seem like something out of a horror movie and often freak parents out. They usually look worse than they are, though, so take a deep breath and follow these simple steps if your child gets a bloody nose:
1. Lean Your Child’s Head Forward, Not Back.
Parents tend to lean their kids’ head backwards with nosebleeds, but the forward lean is actually the way to go.
2. Apply Pressure to the Nostrils for 5-10 Minutes.
Use a tissue to pinch the soft part of the nose just above the nostrils. Make sure the pressure is continuous. Offer your child a book to look at or a toy to hold while you wait for the nosebleed to resolve.
3. If the Bleeding Doesn’t Stop After 10 Minutes of Holding Pressure, Call the Doctor.
PediaTip: Kids who have a bloody nose and are crying often look like they’re gushing blood. This is because the mucus from the crying makes the blood flow even more. If your child has a nosebleed and is crying, take them to a quiet place where they can settle down and you can hold pressure.
Reality Check: When kids have frequent nosebleeds, their parents often worry that they have a bleeding disorder. However, recurrent nosebleeds are more likely to be caused by recurrent nose picking than by a medical condition. That being said, nosebleeds that are difficult to control occasionally indicate a problem, especially if there’s a family history of a bleeding disorder. Let the doctor know if it’s consistently hard to get your child’s nosebleeds under control.
The Bottom Line
Most kids walk independently by 15 months. Children develop at their own pace, though, so try not to hover if your kiddo is taking their sweet time to walk. The pediatrician will evaluate your child’s developmental milestones at every checkup and will let you know if they have any concerns. If you’re worried, take some video of your child and show it to the doctor so they can see what you’re seeing. Any child who limps, has an unusual gait, or refuses to walk because of pain, should get checked out by a doctor, as well. And remember…most nosebleeds are due to “nose mining” (vs. nose trauma or a bleeding disorder) and can be managed by holding pressure for 5-10 minutes.
Celebrities Are Just Like Us!
“I love kids. I was a kid myself, once.”
~Tom Cruise
The Reminders for This Week are the Same as Last Week’s. Get Wise About Them Below…
Limit Your Child’s Whole Milk to 16-24 Ounces Per Day.
Feed Your Child What You Eat, But Cut into Small Pieces.
Steer Clear of Choking Hazards. Get Wise About the Top 10 (Food) Choking Hazards Here.
Brush Your Child’s Teeth Twice a Day (Especially After the Last Meal of the Night) and Have Them Visit the Dentist Every 6 Months (Unless the Dentist Says Otherwise).
Call the Doctor If Your Child Spikes a Fever Above 102.2°FOR If They Develop Any Other Worrisome Symptoms (Such as Lethargy or Poor Feeding).
Continue to Give Your Child a Daily Vitamin D Supplement (600 International Units Per Day).
Keep Your Child in a Rear-Facing Car Seat Until (At Least) 2 Years of Age.
And…That’s a Wrap!
Welcome to Month 12 (Week 2) ofParenting Your Toddler!
Hopefully, your toddler is taking a shine to the whole milk (or to a cow’s milk alternative). Remember to limit their milk intake to 16-24 ounces per day. Why? Because drinking too much whole milk can fill toddlers up and prevent them from getting enough nutrients from their solid foods. It can also be a setup for iron deficiency anemia and constipation.
Parents often complain that their toddler “never eats anything” or eats only “beige foods” (think: mac & cheese and chicken nuggets). As children enter toddlerhood, they tend to develop strong opinions about what they like and what they don’t like.
Get Wiseabout the Top 10 Tips for Managing Picky Eaters (Note: These tips can help any eater at this age).
Insider Info: When children hit the toddler years, their growth rate slows. As mentioned before, kids tend to be at their chubbiest around 6 months (when they’re not very mobile and they’re crushing breast milk or formula and starting solid foods). As children near 1 year of age they burn more calories and become distracted eaters. Toddlers are busy bees and can get restless when they have to sit in their highchair and eat. Keep your expectations low when it comes to how long your toddler can sit in their highchair. 10 minutes is a success at this point, although some kids are able to hang in there a bit longer.
A Word About Multivitamins
The American Academy of Pediatrics (the AAP) says most children don’t need a multivitamin as long as they’re eating a “well-balanced diet” and growing properly.1
But What Does “Well-Balanced” Mean, Exactly? Well-balanced doesn’t mean that your child has to have a perfect diet. Even kids who turn up their noses at fruits & veggies, don’t usually need a multivitamin. The kids who typically require a multivitamin are:
Vegans and vegetarians.
Why? Because they’re at risk for a vitamin B12 deficiency.
Kids who were born prematurely or who have a chronic medical condition.
Children who refuse to eat ANY fruits or veggies and who reject ALL forms of calcium. This isn’t very common, though.
PediaTip:Ask your child’s doctor for their take on whether your little one needs a multivitamin.
Even if a child (age 1 year or older) doesn’t require a multivitamin, the AAP still recommends that they take a daily vitamin D supplement (with 600 international units of vitamin D in it).
PediaWise Pick:A good stand-alone vitamin D option is Ddrops Booster Liquid Vitamin D3. I like this product because 1 drop contains the entire 600 international units of vitamin D.
In addition, keep a loose eye on your child’s calcium intake. Toddlers (1-3 year-olds) require 700 milligrams (mg) of calcium per day. 16-24 ounces (i.e. 2-3 cups) of whole milk per day should cover your child’s basic calcium needs. Yogurt and cheese are good sources of calcium, as well.
Disease Spotlight: Reflux in Toddlers
In rare cases, picky eating in toddlers is due to Gastroesophageal Reflux Disease (GERD).
As a review, “GER” (Gastroesophageal Reflux) is a condition in which the acidic juices from the stomach flow backwards into the esophagus (the food tube). GER is a common phenomenon in infants and is called Gastroesophageal reflux disease (GERD) when it causes significant symptoms.
Although the majority of kids outgrow their reflux by 1 year, some cases persist into the toddler years (and beyond).
What are the Symptoms of GERD in Toddlers?
As you may remember, infants with GERD spit up frequently, arch their backs, and are super fussy. Toddlers, however, show symptoms of GERD in more subtle ways. Namely, they:
Eat super slowly.
Complain of stomachaches (especially after eating).
Vomit occasionally out of the blue.
Have trouble gaining weight (despite wanting to eat).
Subconsciously regulate their portion sizes by grazing during the day or by declaring they’re full sooner than expected. Or they may simply avoid eating even though they seem hungry.
Additional Symptoms Include:
Dental Erosions:Dental erosions develop when the stomach acids reach the mouth and wear down the enamel. The child’s dentist may be the first to notice them.
Wheezing, a Chronic Cough, or a Hoarse Voice:In this case, the stomach juices irritate the airway. GERD can also trigger asthma flare-ups in kids with pre-existing asthma (or reactive airway disease).
Get Wise About the Top 5 Tips for Managing Gastroesophageal Reflux Disease (GERD) in Toddlers.
The Bottom Line
Toddlers are notorious for being picky eaters. Picky eating is usually just a phase and is rarely due to an underlying disorder (such as GERD). Reach out to your child’s doctor, though, if you’re concerned about your little one’s growth or if they exhibit any of the reflux symptoms described above.
“My mother’s menu consisted of two choices: Take it or leave it.”
~Buddy Hackett
The Reminders for This Week are the Same as Last Week’s. Get Wise About Them Below…
Limit Your Child’s Whole Milk to 16-24 Ounces Per Day.
Feed Your Child What You Eat, But Cut into Small Pieces.
Steer Clear of Choking Hazards. Get Wise About the Top 10 (Food) Choking Hazards Here.
Brush Your Child’s Teeth Twice a Day (Especially After the Last Meal of the Night) and Have Them Visit the Dentist Every 6 Months (Unless the Dentist Says Otherwise).
Call the Doctor If Your Child Spikes a Fever Above 102.2°FOR If They Develop Any Other Worrisome Symptoms (Such as Lethargy or Poor Feeding).
Continue to Give Your Child a Daily Vitamin D Supplement (600 International Units Per Day).
Keep Your Child in a Rear-Facing Car Seat Until (At Least) 2 Years of Age.
And…That’s a Wrap!
Welcome to Month 12 (Week 1) of Parenting Your Little One!
Even though 12-month-olds may only be able to say “Mama,” “Dada,” and one other word, they’re often finding their “voice” in other ways. For example, they may express their frustration by throwing food on the floor, pulling their parent’s hair, or rejecting their diaper change. While having a strong voice is a good thing (in the long run), parents don’t usually expect this much opposition so early on.
The American Academy of Pediatrics (the AAP) recommends that 1-to-2 year-olds get 11-14 hours of shuteye per day (including naps). Naps may get tricky in the upcoming year. Some kids love their 2 naps a day, while others have major FOMO and start refusing their second nap. We’ll talk about this (and what to do about it) as the year unfolds.
Feeding:
Your child can now drink whole milk (limited to 16-24 ounces per day) and eat the foods that you eat (in manageable bites). This will be the standard fare going forward. Because 1-year-olds are in constant motion, feeding issues tend to crop up at this stage. Don’t worry, I’ll provide tips on how to manage them along the way.
Healthy Teeth:
As children get deeper into the toddler years, they often insist on brushing their teeth by themselves. While seeking independence is great and all, toddlers aren’t the most thorough when it comes to toothbrushing. If your child insists on wielding the toothbrush, buy 2 toothbrushes: one for them to hold and one for you to hold. Let your child brush first, then swoop in with the second brush to catch any areas that were missed.
Common Question: How Many Baby Teeth Do We Have Again?
Humans have 20 baby (primary) teeth and 32 adult teeth.
Here’s a Review of the Baby Tooth Breakdown:
8 incisors (4 central incisors and 4 lateral incisors).
4 cuspids (aka canines or eye teeth).
4 one-year molars.
4 two-year molars.
There’s a vague order to the way we gain (and lose) our teeth. Babies typically get their front two bottom teeth first, followed by their top 4 front teeth. The picture below shows the general order and timing of when teeth come in (although there’s a lot of variation among kids).
Insider Info:All baby teeth are typically in by 3 years of age. By then, teething should be a thing of the past.
Get Wise About the Top 10 Tips for Preventing Cavities in Toddlers.
No one tells you that the Terrible Twos actually start around 1 year of age and may extend into year 3 and beyond.
Tantrums, though annoying at times, are not all bad. They give your child a chance to blow off steam and can be pretty amusing. Make sure to get video footage while you can.
Here are 5 Tips for Managing Toddler Tantrums
1. Offer Choices, But Not Too Many.
Kids, like most people, want to be in control. By offering your child choices, you’ll give them a sense of independence and a feeling that they’re in charge. In addition, you’ll avoid getting blamed for whatever decision your child makes, because they’re the one who made it.
Offer 2 choices max so your kiddo doesn’t get too overwhelmed. Also make it clear that some things are not negotiable. For example, your child has to buckle up in their car seat no matter what.
Here’s an Example of How to Offer Choices: If your child makes a fuss about getting dressed, you can say, “You have to get dressed now. Do you want to start with your socks or with your pants?” Hold up each item as you’re naming it.
Although this tactic may fly over your kid’s head a bit during the early toddler days, they understand more than you think and will eventually get the hang of it.
2. Don’t Give the Tantrum Too Much of YOUR Energy.
Kids love to get intense reactions — both positive and negative — from their parents. Don’t feed the beast by giving the tantrum too much of your energy. Remain calm (easier said than done) and take a breath (or two) so you can respond intentionally (vs. reactively).
3. Redirect.
Toddlers are highly distractible. Use this to your advantage. If you see a meltdown coming on, try to preempt it by shifting your child’s attention to something else (like a toy).
4. Try to Get to the Bottom of the Tantrum (But Don’t Bother Digging Too Deep).
Quickly run through a mental checklist of what might be upsetting your child: Are They Hungry? Tired? Bored? Overstimulated? Getting Sick? In Need of a “Good Cry”?You don’t have to go “all Freud” on the situation; just take a few seconds to consider the potential tantrum triggers.
5. Put Your Child in a Safe Place and Wait Until the Tantrum is Over.
With some tantrums, kids are off to the races and there’s no turning back. In this case, your child may need to get the tantrum out of their system. Give them the space to do so.
Bonus Info: Does Your Little One Have Oscar-Worthy Tantrums OUTSIDE of Your Home? Get Wise About the Top 5 Tips for Managing Public Tantrums.
Ok. Now, Let’s Move Onto Some General Parenting Tips and Go Over My Top 10 Tips for Parenting Toddlers (PediaWise-Style). Get Wise About Them Below…
Let’s be honest, a lot of parenting is making sh*t up on the fly. There’s no surefire guide to follow or checklist to complete (unfortunately). Kids will, however, quickly alert you to your strengths and weaknesses (especially the latter). Here are a few things I’ve learned (through trialand error) along the way:
1. Be Adaptable.
Parenting isn’t static. Just when you feel like you’ve mastered one part of parenting, your child will find a new challenge to throw at you. Be flexible and learn to pivot so you can weather the parenting storms.
2. Give More Space Than You Think You Need To.
While we all love to hover, correct, and cajole, give your child the space to make mistakes and learn things on their own. This anti-helicopter approach requires that we bite our tongues and think about the long-term goal – to raise resilient kids who can think for themselves.
3. Parent Intentionally (vs.Reactively).
All too often, we find ourselves reacting to a situation and parenting out of emotion, rather than giving a problem space. When things go sideways, try to create a pause between your emotions and your reaction. If you’re seeing red, take care of yourself first, before stepping in to “parent.”
Mantras can help in this situation. For example, you can tell yourself things like: “We’re ok,” “Breathe,” “Our relationship is more important than this,” “I choose love,” or whatever else speaks to you.
4. Give Choices (But Not Too Many).
As mentioned above, providing choices is a great way to empower kids. It’s also a loophole that gets parents out of being the “bad guy.” Offering too many choices too often, however, can overwhelm a child and set up an expectation that everything is negotiable. This will come back to bite you in the you-know-what when your child goes to school and doesn’t understand why the rules aren’t up for debate.
5. Take Time to Play.
There’s a great book called “Playful Parenting” by Lawrence J. Cohen that emphasizes the importance of getting on the floor and playing with our children. If we’re honest, though, most of us can only play “pat-a-cake” for so long.
Luckily, this book espouses quality over quantity. Try to create 10-15 minutes of “connect time” with your child each day during which they get to dictate the play and you’re an engaged participant (i.e. you’re not looking longingly at your smartphone).
6. Self-Care is Key.
Back in the day, children “were seen and not heard.” Today, parents seem to be a cross between Sherpas and unpaid Uber drivers. We’re forever carting our kids around to various play dates and activities, talking about our children, and worrying about them.
Where’s the All-Important “Me” Time?! For some reason, “Me” time has become a guilty pleasure rather than an act of self-care. If you give everything you have to your child, you’ll get depleted, and may even start to feel a bit resentful. So, make sure to block off some time for yourself, both your sake and the sake of your family.
7. Don’t Listen to All the Noise.
Opinions are a dime a dozen when it comes to parenting. Everyone wants to put their 2 cents in, and it can be hard to trust yourself and to feel like you’re doing anything right. Plus, it’s natural to want to compare your child to other kids to see how they “measure up.” This, of course, is a losing battle, because there’s always someone “better” at something and you don’t necessarily have all of the facts about the others kids’ ages, medical histories, family histories, and struggles.
So, try to block out the noise, let go of the comparing mind, and focus on what’s most important to you and your family.
8. Love Your Child, But Avoid Getting Too Enmeshed With Them.
There’s nothing like the love between a parent and a child. Because of this bond, it’s easy to start experiencing your child’s highs and lows as if they were your own. Try to get off the emotional rollercoaster, though, and remember that your child has their own journey to travel. This will enable you to be the anchor (i.e. the grown-up) when your little one is caught up in a sea of emotions.
9. Trust Yourself.
This can be tough because there’s no rulebook for raising kids and we often look outside of ourselves to see if we’re doing it right. Remember that you know your child better than anyone.
10. Don’t Be Too Hard on Yourself.
Cut yourself some slack and know that not everything has to be (and won’t be) perfect. As Nelson Mandela once said: “I never lose. I either win or I learn.”1 If you make a mistake or have a bad day, don’t beat yourself up about it, just learn from the experience.
Bonus Tips:
Don’t Put Your Partner (Completely) on the Back Burner.
Ask For Help When You Need It.
Know That What Works For Another Family Might Not Work For Your Family, And Vice Versa.
Understand That Kids Respond Differently to Different Parenting Techniques. If you have more than one child, take the time to understand your kids’ different temperaments and try to figure out which parenting techniques work best for each of them.
Set Limits and Clear Boundaries: Routines and boundaries are soothing for children. Although kids may seem like they want to be in complete control, gaining too much power actually scares them and makes them feel like the world is a topsy-turvy place. Children need clearly defined boundaries, but they also need freedom within those boundaries to explore and make mistakes.
A Word for Divorced Parents:
Try to get on the same page with parenting if possible. If it’s not in the cards, though, don’t sweat it too much. Your child will learn to accept that there are different rules in the different homes (if that’s the case). As long as the separate sets of rules are consistent in each environment, things will work out. In addition, try to avoid bashing your ex in front of your kiddo and do your best to keep any arguments on the down-low. Kids tend to model what they see and are smart about reading the energy between their parents.
The Bottom Line
Be kind to yourself, expect parenting to be messy, and look for the humor in it all.
“The most important thing she’d learned over the years was that there was no way to be a perfect [parent] and a million ways to be a good one.”
~Jill Churchill
Check Out the Reminders for This Week Below…
Limit Your Child’s Whole Milk to 16-24 Ounces Per Day.
Feed Your Child What You Eat, But Cut into Small Pieces.
Steer Clear of Choking Hazards. Get Wise About the Top 10 (Food) Choking Hazards Here.
Brush Your Child’s Teeth Twice a Day (Especially After the Last Meal of the Night) and Have Them Visit the Dentist Every 6 Months (Unless the Dentist Says Otherwise).
Call the Doctor If Your Child Spikes a Fever Above 102.2°FOR If They Develop Any Other Worrisome Symptoms (Such as Lethargy or Poor Feeding).
Continue to Give Your Child a Daily Vitamin D Supplement (600 International Units Per Day).
Keep Your Child in a Rear-Facing Car Seat Until (At Least) 2 Years of Age.
And…That’s a Wrap!
Welcome to Month 20 (Week 1) of Parenting Your Toddler!
Although starting preschool may seem like a far-off event, it doesn’t hurt to do a little prep work in advance. Most nursery schools require children to be 2.5 years or older to matriculate. Some insist that children be potty-trained as well, although many schools are lax on this front or will do the potty training for you (which is a nice perk!).
When Thinking About Preschools, It Helps to Do the Following:
Get Tips on How to Do These Things in the Hot Topics Section Below…
Signs of Preschool Readiness
Preschool readiness is more about emotional and social readiness than about being able to recite one’s ABCs. Below are the skills kids need to have (to varying degrees) to make school a success. They should:
Be at Least Somewhat Interested in Going to “Big Kid” School.
Be Able to Separate From Their Parents For a Few Hours. This takes practice. Nursery schools typically ease kids into school. Rather than have school 5 days a week for the entire day, preschools typically offer a few morning-only or afternoon-only sessions per week. As kids get older, they build up their stamina and are able to stay in school longer.
Be Able to Initiate Independent Play and Entertain Themselves (For a Bit).
Be Able to Express Themselves Enough to Get Their Needs Met. This doesn’t mean your child needs to be able to talk in complete sentences. As long as your child can communicate the basics (i.e. when they’re hungry, thirsty, hurt, tired, etc.), you’re golden.
Be Able to (Sort of) Follow Directions.
Finding the Right Preschool for Your Child
Consider These Questions When Looking For a Preschool for Your Child:
What are the Logistics? Logistics are key. Choose a school that’s close by (if possible), especially if your child starts in a half-day program. Why? Because there’s less time than you think between drop off and pick up.
What’s the Student-Teacher Ratio? Ideally, your child’s preschool will have a low student-teacher ratio (i.e. a small number of students assigned to each teacher) so your kiddo can get enough care and attention.
What Does the Outdoor Space Look Like? Is There a Lot of Green Space? Is There a Playground?
What Are the School’s Resources? For Example, Does the Classroom Have Board Books and Cool Educational Toys?
What’s Included in the Curriculum?
What’s the Potty-Training Policy? As mentioned above, some schools require kids to be potty trained before entry, whereas others will do it for the parents. The latter is often helpful because it can be tough to get a child completely potty trained by 2.5 years (the typical entry age for nursery school).
What’s the School’s Health Policy and When Does the School Allow Sick Kids to Return to Class? A strict health policy may mean that your child gets sick less often, but it may also mean they have to stay home with every sniffle.
Does the School Provide Food? If So, What’s the Menu Like?
Are There Any Volunteer Activities for Parents?
What’s the School’s Philosophy?
What’s The Vibe of the School? Do the Teachers Look Happy (or Slightly Annoyed)?
What are the Other Parents Like? Are they laid back or do they already have their kids enrolled in chess clubs and Kumon math classes?
A Word About Montessori Programs
During your search for the right preschool for your child, you may hear about the Montessori style of learning. The Montessori method is rooted in “self-directed activity, hands-on learning, and collaborative play.”1 Instead of “teaching,” the teacher follows the child’s lead and guides their learning. Some parents swear by the Montessori philosophy, while others prefer a more traditional approach.
A Word About Gifted & Talented Programs
All kids have their own unique gifts and talents, but a small percentage of them are recognized as “gifted” and “talented” in the school setting. These children have abilities significantly above the norm in areas such as math, science, language arts, creativity, and leadership.
Precocious kids can take standardized tests to determine if they qualify for a “gifted and talented” educational program. However, the National Association for Gifted Children recommends that kids wait until they’re at least 6 years old to take these tests (although some schools and private evaluators will test students earlier). FYI:The testing can get pricey (think: hundreds of dollars) so if your child ends up doing it, you want to time it right.
Reality Check: Only 6% of K-12 public school students are enrolled in gifted and talented programs in the U.S.2
Prepping Your Child for Preschool
Although it’s hard to predict whether your child will walk into preschool like they own the place or desperately cling to your leg as you try to leave, there are a few things you can do to help prepare them for their first day. Here are some tips:
Ask the Teacher If Your Child Can Spend a Little Time in the Classroom Before Their First Day of School.
Arrange a “Playdate” With Another Child in the Class Before School Starts. The teacher can tell you which student might be a good fit, personality-wise, for your child.
Get Your Child Excited About School Supplies.I mean, who doesn’t love school supplies?! They’re fun and make kids feel super grown-up.
Expect Some Jitters During the First Few Weeks. The transition to school is tough for many kids (and their parents). Have faith that it will work out in time.
Play it Cool. Remain upbeat but avoid being overly hyped and animated. This will just stress your kid out even more.
Make Sure to Get the School Health and Dental Forms Filled Out the Summer Before Your Child Starts School (If They’re Starting in the Fall).
The Bottom Line
Many parents view preschool as a critical step on their child’s path to future success and happiness. Although it helps to be intentional about the application process and to find a school that’s the right fit for your family, it doesn’t have to be perfect. It’s more important to find a school that’s nurturing (and nearby!) than a school whose alums all went to Harvard.
“Being a parent is like folding a fitted sheet, no one really knows how.”
~Unknown
The Reminders for This Week are the Same as Last Week’s. Get Wise About Them Below…
Limit Your Child’s Whole Milk to 16-24 Ounces Per Day.
Feed Your Child What You Eat, But Cut into Small Pieces.
Steer Clear of Choking Hazards. Get Wise About the Top 10 (Food) Choking Hazards Here.
Brush Your Child’s Teeth Twice a Day (Especially After the Last Meal of the Night) and Have Them Visit the Dentist Every 6 Months (Unless the Dentist Says Otherwise).
Call the Doctor If Your Child Spikes a Fever Above 102.2°FOR If They Develop Any Other Worrisome Symptoms (Such as Lethargy or Poor Feeding).
Continue to Give Your Child a Daily Vitamin D Supplement (600 International Units Per Day).
Keep Your Child in a Rear-Facing Car Seat Until (At Least) 2 Years of Age.
And…That’s a Wrap!
Welcome to Month 22 (Week 2) of Parenting Your Toddler!
As your child learns about the function of different tools and toys, they’ll start to get more creative about their play. Toy kitchens, water tables, pretend lawnmowers, and plastic cellphones become fodder for imaginative play at this age. Play is critical for development, but parents often worry when their kids engage in more “violent” forms of play. This is usually a “boy thing,” but not always.
Get Wise about “violent” pretend play and what the research says about it in the Hot Topics below.
“Violent” Pretend Play and Toy Weapons
Allowing children to play with toy weapons is a hotly debated topic in the U.S. and abroad. Back in the day, BB guns were all the rage and “Cops and Robbers” was a popular childhood game.
With school shootings on the rise, however, the image of young children “shooting” each other with plastic guns can feel “wrong” and elicit fear.
In a 2003 study entitled “Community Norms on Toy Guns,” 66% of the parents polled said they refuse to let their children play with toy guns.1 More recently, there have been cases in which kids were suspended from school for bringing nerf guns and guns made out of Legos to class.2
But parents who have banned toy guns in their homes often lament that their “no-toy-weapon” rule didn’t actually eliminate their child’s interest in “violent” pretend play, it just made them more creative about it. (Think: fashioning guns out of sticks and pieces of toast.)
So, What’s a Parent to Do? Should We Step In and Ban All “Violent” Undertones From Our Child’s Play? Is This Even Possible? Are Children Who Pretend to Shoot Things (Either With a Toy Gun or With a Gun Made Out of Bread) Destined to Be Criminals?
Below are the Top 5 Tips for Addressing “Violent” Forms of Pretend Play:
1. Know the Research and See Play for What it Is.
Believe it or not, the prevailing research says there’s no link between playing with toy weapons in childhood and aggression in adulthood.3
Why? Because kids aren’t actually trying to kill each other when they play with toy weapons. Instead, they’re practicing setting boundaries, solving problems, negotiating rules, and exploring power dynamics (by playing the hero and the villain).
2. Set Boundaries Around the Play, Then Let Your Child Have Freedom Within Those Boundaries.
Allowing your child to play with toy weapons doesn’t mean you’re allowing them to go full-on Lord of the Flies. Set boundaries around your child’s play by creating clearly defined rules that make everyone feel physically and emotionally safe.
Examples of Such Rules Include:
Don’t hit another person with a “weapon.”
No pointing a “weapon” at someone’s face.
If someone says “stop” or gives you the thumbs down, stop immediately.
Switch up the hero and the villain roles so that no one is consistently being cast as the “bad guy” or the victim.
3. Choose Your Toy “Weapons” CAREFULLY.
Not All Toy Weapons Were Created Equal. Therefore, if You DO Decide to Let Your Child Play With Toy Weapons, Follow the Tips Below:
Avoid Realistic-Looking Weapons. Some weapons look like the real deal. Opt for less realistic toy weapons to highlight the fact that they’re fake. For example, pick brightly-colored transparent water guns instead of opaque black water guns.
Say No to Toy Weapons and Homemade Weapons That Could Actually Hurt Someone.BB guns, for example, can cause injuries, as can sharp sticks. Nerf guns, which are also popular, can be dangerous if your kiddo gets hit in the eye with a nerf bullet. When it comes to nerf guns, you can either ban them entirely, insist that your child wear eye protection when using them, or introduce them when your child is older and more mature.
4. Avoid the Shame Game.
When a parent admonishes their child for wanting to be the “bad guy” in a game or for playing with a toy weapon, it doesn’t make the desire to do these things go away. It just makes the feelings go underground and manifest in the form of shame.
Wanting to “play” the bad guy, doesn’t mean your child wants to “be” a bad guy. They just want to explore, push boundaries, and solve problems. Have faith in your child’s “goodness” and know that it’s normal to want to try out ALL of the different roles during play.
5. Ban REAL Firearms In the Home OR, If That’s Not an Option, Make Sure to Lock Them Up.
Research has shown that most kids can’t tell a real gun apart from a realistic fake gun.4 Therefore, having a real gun in the house can be a set-up for an accident. We’ve all heard sad stories in the news about kids who’ve accidentally shot family members or friends. If there’s a real weapon in the house, an accident can happen regardless of whether the kids have been allowed to play with toy guns or not.
The American Academy of Pediatrics (the AAP), therefore, discourages parents from having guns in the home at all. If this isn’t an option, the AAP says guns should be locked away and stored unloaded in a separate location from the ammunition.5 Doing this can make a huge difference, although one study showed that only 34% of gun owners with kids actually take these precautions.6
Bonus Tips
Keep an eye out for red flags during pretend “violent” play (such as being overly aggressive).
Have your child continue to “play out” the different scenarios. For example, if someone gets “shot” with the toy gun, ask what happens next. Is there a funeral? Was the person injured? If so, are you going to take them to the hospital?
Teach your child about the dangers of real guns.
Show your child (through role-playing) that not everything is “black and white.” “Evil” characters can have good in them and vice versa.
Violent video games are a different story than toy weapons and “violent-looking” play. When kids play hours upon hours of violent video games, they’re not “working through things” the way they are when they’re engaging in imaginative play.
In fact, the American Psychological Association considers violent video games a risk factor for aggression because they can desensitize kids to violence and cause them to blur the line between fiction and reality.7 The same goes for inappropriately violent movies.
The Bottom Line
When it comes to toy weapons and “violent” play in the home, go with your gut and do what feels right for your family. And don’t forget that kids naturally learn and grow through play, regardless of whether they want to be the “good guy” or the “bad guy” that day.
“Today you are You, that is truer than true. There is no one alive who is Youer than You.”
~Dr. Seuss
The Reminders for This Week are the Same as Last Week’s. Get Wise About Them Below…
Limit Your Child’s Whole Milk to 16-24 Ounces Per Day.
Feed Your Child What You Eat, But Cut into Small Pieces.
Steer Clear of Choking Hazards. Get Wise About the Top 10 (Food) Choking Hazards Here.
Brush Your Child’s Teeth Twice a Day (Especially After the Last Meal of the Night) and Have Them Visit the Dentist Every 6 Months (Unless the Dentist Says Otherwise).
Call the Doctor If Your Child Spikes a Fever Above 102.2°FOR If They Develop Any Other Worrisome Symptoms (Such as Lethargy or Poor Feeding).
Continue to Give Your Child a Daily Vitamin D Supplement (600 International Units Per Day).
Keep Your Child in a Rear-Facing Car Seat Until (At Least) 2 Years of Age.
And…That’s a Wrap!
Welcome to Month 22 (Week 4) of Parenting Your Toddler!
As you may remember from the baby PediaGuide articles, kids get roughly 8-10 viral infections per year. Now that your child is almost 2, you’re probably well-versed in colds and may feel like your child always has a cold, is getting over a cold, or is about to get a cold.
Toddlers don’t feel great with colds, but they tend to weather them better than infants since their airways are bigger.
Toddlers with underlying reactive airway disease (a potential precursor to asthma) may wheeze or have trouble breathing with colds. If your child has this condition, then you’re probably becoming a pro at recognizing when they need an albuterol treatment at home (vs. care in the ER).
Hopefully your kiddo is a fan of sleep. Ideally, they should be sleeping through the night (for 10-12 hours straight) and taking 1-2 naps per day.
Teething, colds, and travel are common disruptors of sleep. If your child’s sleep schedule gets thrown off by one of these (or by something else), try not to get sucked into bad habits (such as rocking your kiddo to sleep) for more than a week or two. Why? Because then you’ll have to spend some time and energy undoing them.
Diet:
Continue to feed your child a variety of foods. Work on introducing new foods into the rotation and avoid choking hazards. At the 2-year mark, you can switch your child from whole milk to a lower-fat milk (2%, 1%, or skim) as long as their doctor says it’s okay.
Disease Spotlight: The Common Cold Revisited
What Exactly Is a Cold, Again?
A cold is a viral infection that causes a runny nose and/or nasal congestion. The runny nose and nasal congestion may be preceded by a fever and a sore throat. Colds are most commonly caused by rhinoviruses, but they can be caused by other viruses, as well.
When Do Colds Usually Occur?
Colds can occur at any time of year, but they’re most prevalent in the fall and winter.
How are Colds Spread?
Colds are typically spread through airborne droplets that are coughed or sneezed into the air by someone who’s sick. They can also be spread through hand-to-hand contact or by touching an object (such as a doorknob) that’s been contaminated with the virus. This is why doctors urge their patients to cough & sneeze into their elbows and wash their hands frequently during cold & flu season.
How are Colds Diagnosed?
Doctors usually diagnose colds based on the patient’s symptoms. No other testing is needed.
Insider Info: If your child has a cold, don’t be weirded out if the doctor holds a stethoscope up to their nose during the physical exam.
What’s the Doctor Doing In this Case? They’re listening for “transmitted upper airway” sounds. Transmitted upper airway sounds are funky (yet benign) sounds commonly heard with colds. These sounds come from the nose rather than from the lungs.
Can Colds Be Treated With Antibiotics or Other Medications?
No. Because colds are caused by a virus, kids, unfortunately, have to ride them out.
In the Meantime, You Can Offer “Supportive Care” By:
Running a Cool-Mist Humidifier In the Room While Your Child is Sleeping: Cool-mist humidifiers help keep the skin lining the nasal passages moist and the mucus loose.
PediaTips:
Be sure to clean the humidifier daily (see the manufacturer’s manual) to prevent the growth of mold and bacteria.
Avoid hot-water vaporizers. Why? Because they can cause burns.
You Can Also…
Keep Your Child Hydrated and Give Tylenol or Ibuprofen as Needed for Fevers. Call the Doctor for Fevers Above 102.2°F.
Try Saline Nose Drops: Saline nose drops are basically just sterile saltwater. Squirt 2-3 drops into each of your child’s nostrils (ideally 15-20 minutes before feeds and bedtime). The salt in the drops will help dry up the mucus.
PediaTip: Make sure to get the non-medicated (“drug-free”) version of the saline nose drops (as in the PediaWise Pick above). You can also make your own normal saline at home by mixing ½ teaspoon of non-iodized salt in 8 ounces of distilled or boiled water.
Insider Info: Saline nose drops are hit or miss with toddlers. Most toddlers hate having things squirted up their noses, but a small minority of them will let their parents do it. You can try to coax your kiddo into using them by asking them to “help” administer them. If you end up having to wrestle your little one to the ground every time you try to put the drops in their nose, though, don’t bother with them.
In Addition to the Above Tips, Be On the Lookout For “Concerning Symptoms.”
What “Concerning Symptoms” Are You Talking About?
Concerning Symptoms Include:
Trouble Breathing: Most toddlers do not have trouble breathing with colds. However, as mentioned above, colds can trigger wheezing and respiratory distress in kids with underlying reactive airway disease. These children may need albuterol treatments (to open up their airways) or even a course of oral steroids (to reduce the airway inflammation). If your child doesn’t have reactive airway disease but is struggling to breathe, they may have something more serious than the common cold (like pneumonia).
The Bottom Line: Call the doctor (or 911) if your child is having trouble breathing.
Clear Snot That Turns Into Green Snot: Green snot can be a sign of a bacterial sinus infection. Although bacterial sinusitis isn’t super common in toddlers, it can happen (especially if the nasal congestion has been going on for a while).
New or High Fevers.
These Include:
Fevers that go away and come back.
Fevers that suddenly appear after several (3-4) days of illness.
High fevers (e.g. fevers over 102.2°F).
Why are These Fevers a Problem? Because they can be a sign that a bacterial infection (such as an ear infection, sinusitis, or pneumonia) is developing on top of the original viral infection. Call the doctor if your child develops one of these types of fevers.
A Word About Cough & Cold Medications
An mentioned in previous PediaGuide articles, the American Academy of Pediatrics (the AAP) says cough and cold medications should not be used in kids under 6 years of age (although some experts say 4 years).1
Why’s That?Because they don’t seem to be all that useful in this age group and they’ve also led to a small number of fatal poisonings in young children (most of which occurred in children under 2 years). Reality Check: This is super rare, but not worth messing around with.
In addition, watch out for herbal remedies and supplements. Although they may sound like a good idea and tout promising healing properties, they’re not well regulated by the FDA (the Food and Drug Administration).
Also know that Vicks VapoRub is not approved for children under 2 years.2
Why? Because one of the ingredients, camphor oil, can get absorbed through the skin and cause seizures in babies and young toddlers.
A Word About Environmental Allergies
A runny nose and nasal congestion inchildren under 1 is almost always due to a cold. However, as children get older, environmental allergies can come into play. If your child tends to get a runny nose during specific times of the year or around certain environmental allergens (such as cats), let the doctor know.
Insider Info: A child is more likely to have environmental allergies if there’s a family history of them.
Repeat Tips on How to Minimize Infections:
Practice Good Handwashing and Have Hand Sanitizers at the Ready(Especially During Cold & Flu Season).
Teach Your Child to Cough and Sneeze Into Their Elbow (vs. Into Their Hand).
Educate Your Child About Germs and Personal Space.
Avoid “Sick Contacts.” Postpone play dates with sick kids and keep a polite distance from anyone with a hacking cough or a runny nose.
Keep Your Child Up-to-Date on Their Immunizations.
Relax. Do what you can but let go of the rest. Germs are a part of life and, in the long run, will help your child build up their immunity.
The Bottom Line
Although colds aren’t fun for anyone, toddlers tend to do pretty well with them. That being said, let the doctor know if you have any concerns about your child’s cold or if they develop one (or more) of the red flag symptoms described above.
And…Breathe….
And, Here’s a Quote…
“Children have never been very good at listening to their elders, but they have never failed to imitate them.”
~James Baldwin
The Reminders for This Week are the Same as Last Week’s. Get Wise About Them Below…
Limit Your Child’s Whole Milk to 16-24 Ounces Per Day.
Feed Your Child What You Eat, But Cut into Small Pieces.
Steer Clear of Choking Hazards. Get Wise About the Top 10 (Food) Choking Hazards Here.
Brush Your Child’s Teeth Twice a Day (Especially After the Last Meal of the Night) and Have Them Visit the Dentist Every 6 Months (Unless the Dentist Says Otherwise).
Call the Doctor If Your Child Spikes a Fever Above 102.2°FOR If They Develop Any Other Worrisome Symptoms (Such as Lethargy or Poor Feeding).
Continue to Give Your Child a Daily Vitamin D Supplement (600 International Units Per Day).
Keep Your Child in a Rear-Facing Car Seat Until (At Least) 2 Years of Age.
And…That’s a Wrap!
Welcome to Month 24 (Week 1) of Parenting Your Toddler!
Now that your child has hit the 2-year mark, they’re (hopefully) in a good routine when it comes to sleep. The majority of kids are sleeping through the night at this age and taking 1 or 2 naps per day.
As mentioned in prior PediaGuide articles, nightmares and night terrors become a thing during the toddler years. Nightmares occur during REM (dream) sleep and are typically remembered, whereas night terrors (which are freaky to witness) occur in a deeper stage of sleep and are thankfully not remembered (at least by the kids). You can promote healthy sleep in your child by creating (and following) a dependable sleep routine and powering down all electronic devices an hour or two before bed (as “blue” light tends to disrupt sleep).
In Addition, Get Wise About Snoring In Toddlers and What It Can Mean.
Nightmares & Night Terrors Revisited
As mentioned above, nightmares are bad dreams that occur in the second half of the night during REM sleep (the dream portion of sleep). Kids are frightened by these dreams and can recall many of the terrifying details. With some coaxing, they (usually) go back to sleep.
Night Terrors, on the other hand, aren’t dreams per se, but represent a “fear response” that’s evoked in some kids when they transition from deep sleep to a lighter stage of sleep. Night terrors take place during the first third of the night, roughly 2-3 hours into sleep.
Night terrors can be jarring for the toughest of parents because kids appear agitated and often scream bloody murder during them. During a night terror, the child may have a blank expression on their face and not even recognize their parents. Fortunately, kids go back to sleep pretty easily after a night terror and wake up having no memory of the episode.
PediaTrivia: Night terrors tend to run in families. In fact, 80% of kids with night terrors have a family member who either had night terrors or were prone to sleepwalking.1 Sleepwalking (like night terrors) occurs during non-REM sleep. Because of this, sleepwalkers don’t usually remember their sleepwalking episodes, either.
Managing Nightmares
Nightmares are Usually Nothing to Worry About and Lessen Over Time. Here are Some Tips to Manage Nightmares:
Listen and Empathize: Allow your child to talk about their nightmare (when they’re verbal enough to do so). Reassure them that the dream “wasn’t real,” but avoid perseverating on this fact. Even though the nightmare wasn’t real, it felt real and you don’t want to get into an existential debate about it in the middle of the night. You also don’t want your child to think you’re an out-of-touch adult who just doesn’t understand.
Empower Your Child: If your kiddo insists that a monster is under their crib or bed, check with a flashlight. Then come up with a “plan” to manage the monster if they come back. For example, your toddler can “defend” themselves against it or make friends with it. When your child is a bit older, you can teach them to take control of the nightmare by rewriting its ending or having them draw a picture of it and tearing it up.
Maintain a Predictable and Calming Bedtime Routine.
Invest in a Nightlight.
Offer Your Child a Transitional Object Such as a Teddy Bear or a Blankie.
Hang a Dreamcatcher Near Their Crib or Bed.
Safety Tip: Make sure the dreamcatcher is out of reach and doesn’t have any loose strings dangling off it or other pieces that your child could tug on.
Teach Your Child Mindfulness and Relaxation Techniques.
Resist the temptation to sleep with your child after the nightmare.
Why? Because you may end up falling into a co-sleeping habit that’s hard to break. Plus, it may send your child the message that they need your protection and can’t handle the nightmare on their own.
If your child has a recurring nightmare that causes them stress, probe a bit deeper to see if the dream is a manifestation of some deeper fear or anxiety. Most bad dreams are just dreams (sorry Freud!) but let the pediatrician know if there’s a pattern to the nightmares especially if they seem to be affecting your child’s overall wellbeing and mood throughout the day.
Managing Night Terrors
Night terrors are a bit trickier to manage than nightmares because they’re so disturbing to witness and the child has no idea what’s going on. Although night terrors are benign, it can be unnerving for parents to see their child seemingly possessed. Here are a few tips to manage night terrors:
Reduce Stress and Fatigue: Night terrors are often triggered by stress or fatigue, so try to minimize both at home.
Consider Waking Your Child Up Before the Night Terror Occurs:Some parents have had success waking their child up 15-30 minutes before the expected episode in an effort to disrupt the sleep cycle. Although waking a child up usually sounds like a bad idea, it can be helpful in this case.
Caution: Waking a child up during the sleep terror, has not been proven to be helpful, and can actually be disorienting and anxiety-provoking for the child.
Remind Yourself That Your Little One Won’t Remember Their Night Terror, No Matter How Intense It Looks.
The Bottom Line:Sleep issues are common during childhood and tend to wax and wane over time. Kids tend to outgrow sleep terrors by age 12 and nightmares generally dissipate with age but don’t fully disappear.
The Snoring Toddler
Some kids snore like it’s nobody’s business. Although snoring is usually a transient thing caused by nasal congestion, it can be a sign of a more worrisome problem called obstructive sleep apnea.
What’s Obstructive Sleep Apnea?
Obstructive sleep apnea (OSA) is a type of disordered (irregular) breathing that occurs during sleep. In adults, it’s often caused by being overweight, but in kids it’s primarily due to enlarged tonsils and over-sized adenoids.
Note: Obesity can be a risk factor for OSA in kids, too.
Quick Anatomy Lesson:You can see your child’s tonsils if you look at the back of their throat. They look like two pink oval-shaped tissues. Unlike the tonsils, the adenoids (a patch of tissue that sits deep in our nasal cavity), are hidden from view. For the adenoids to be visualized, an ear, nose & throat doctor (an ENT) needs to look into the child’s nose with a fiberoptic scope. The fiberoptic scope is usually best tolerated by older children. Because of this, ENTs often order a neck x-ray to evaluate the adenoids of younger children.
PediaTrivia:
Even though we use the plural term for “adenoids,” there’s only 1 adenoid. There are 2 tonsils, however. Hopefully this will be a Final Jeopardy question that you can rock one day!
What Do Tonsils and Adenoids Have to Do With OSA in Kids, Again?
Kids with Obstructive Sleep Apnea have tonsils and/or adenoids that are so big that they partially obstruct the upper airway during sleep. 1-5% of kids in the U.S. suffer from this condition.2 Although OSA can occur in children of any age, it’s most common in kids 2-6 years.
What are the Symptoms of Obstructive Sleep Apnea in Toddlers?
OSA Symptoms Include (But Aren’t Limited To):
Loud snoring.
Pauses in breathing during sleep.
Making loud gasps, choking sounds, and chortles while slumbering.
Restless sleep.
Trouble waking up in the morning.
Mouth breathing (i.e. breathing heavily through the mouth) during the day and while asleep.
Insider Info: Obstructive sleep apnea can mimic ADHD (Attention Deficit Hyperactivity Disorder) in older kids by making them appear hyper and unfocused. Doctors will often rule out OSA before they diagnose a child with ADHD.
Why is Obstructive Sleep Apnea a Problem?
OSA not only leads to poor sleep but, when left untreated, it can cause behavioral problems, poor school performance, heart issues, stunted growth, and developmental delays.
How is Obstructive Sleep Apnea Diagnosed and Treated?
Snoring in children often comes to light during a routine checkup when a parent offhandedly mentions that their child snores frequently. This statement causes the pediatrician’s ears to perk up.
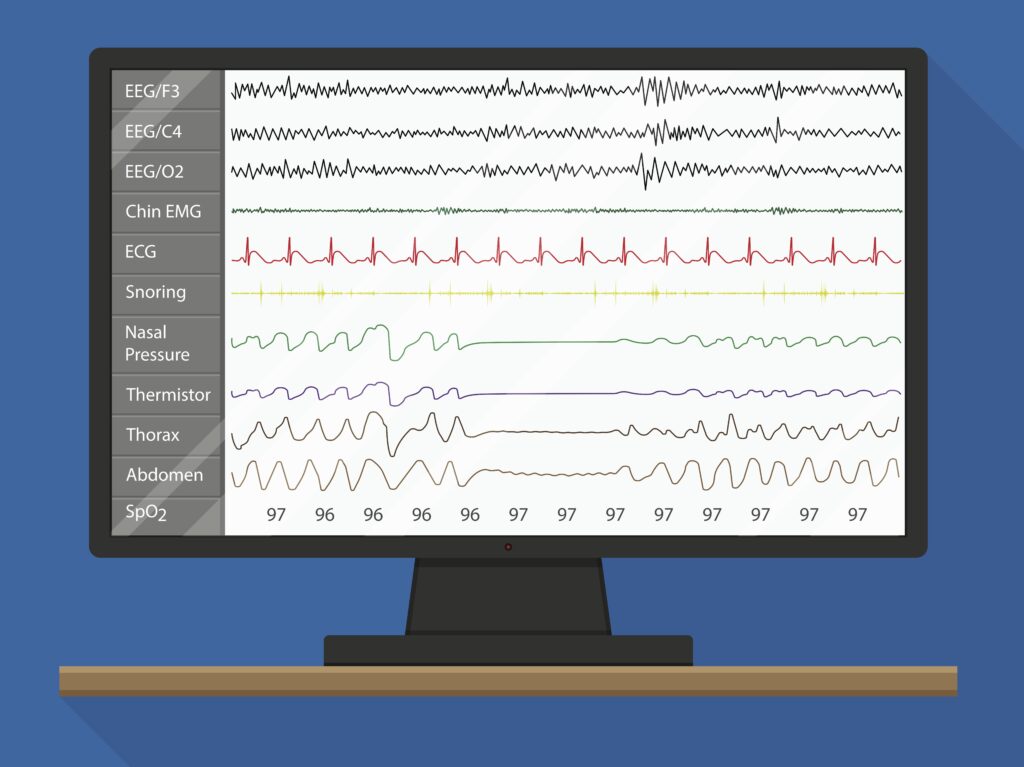
If your child is a snoring machine, the doctor may recommend that they get a sleep study (fancy name: nocturnal polysomnography). For the sleep study, your child will have a bunch of electrodes glued to their head (in a non-painful way) and will spend the night in the hospital (with a parent) while experts monitor their sleep.
Kids who are found to have obstructive sleep apnea on the sleep study are then sent to an ENT. If your child is found to have severe OSA (on the sleep study) and enlarged tonsils/adenoids on the ENT’s physical exam, then surgery is the most likely next step.
Severe cases of Obstructive Sleep Apnea require either the complete removal of the adenoids and the tonsils (aka an adenotonsillectomy) or just a portion of them. Adenotonsillectomies are fairly common and can be life-changing for a child. The recovery period is about 2 weeks depending on how much of the tonsils and adenoids are taken out.
Get Wise(r) About Adenoidectomies and Tonsillectomies.
For mild to moderate cases of OSA, the ENT may take a “watchful waiting” approach and prescribe a steroid nasal spray to reduce the inflammation in the nose, especially if there’s a history of seasonal allergies or environmental allergies. Wearing a mask at night that delivers positive airway pressure (via a CPAP or BiPAP machine) is also an option.
PediaTip: If you think your child has Obstructive Sleep Apnea, take a video of them sleeping. In some cases (like in my daughter’s case), the OSA is so obvious and pronounced that the ENT will skip the sleep study and go straight to surgery.
The Bottom Line
Most snoring is caused by nasal congestion from a cold or allergies. However, if your child snores regularly (3+ nights per week), has pauses in their breathing during sleep, and seems chronically tired let the doctor know.
Celebrities Are Just Like Us!
“A 2-year-old is kind of like having a blender, but you don’t have a top for it.”
~Jerry Seinfeld
The Reminders for This Week are Nearly the Same as Last Week’s (Except for the New Milk Recommendation). Get Wise About Them Below…
Limit Your Child’s Whole Milk to 16-20 Ounces Per Day (Starting at 2 Years of Age).
Feed Your Child What You Eat, But Cut into Bite-Sized Pieces.
Steer Clear of Choking Hazards. Get Wise About the Top 10 (Food) Choking Hazards Here.
Brush Your Child’s Teeth Twice a Day (Especially After the Last Meal of the Night) and Have Them Visit the Dentist Every 6 Months (Unless the Dentist Says Otherwise).
Call the Doctor If Your Child Spikes a Fever Above 102.2°FOR If They Develop Any Other Worrisome Symptoms (Such as Lethargy or Poor Feeding).
Continue to Give Your Child a Daily Vitamin D Supplement (600 International Units Per Day).
Keep Your Child in the Rear-Facing Position in Their Car Seat Until They Exceed the Height and Weight Restrictions Outlined by the Manufacturer.




































{kind=link}
{kind=link}